Overview
Vaginal hysterectomy is removal of the uterus through the vagina without any abdominal incisions. It is the preferred approach for hysterectomy when feasible, and is often performed as part of prolapse repair surgery. It may be combined with anterior repair, posterior repair, and apical suspension procedures.
Indications
- Uterine prolapse requiring surgical treatment
- Abnormal uterine bleeding
- Symptomatic fibroids (when vaginal approach is feasible)
- Completed childbearing with symptomatic pelvic organ prolapse
Advantages
- No abdominal incisions or scars
- Often a shorter recovery than open abdominal hysterectomy, although individual recovery varies
- Shorter hospital stay
- Lower postoperative pain
The Procedure
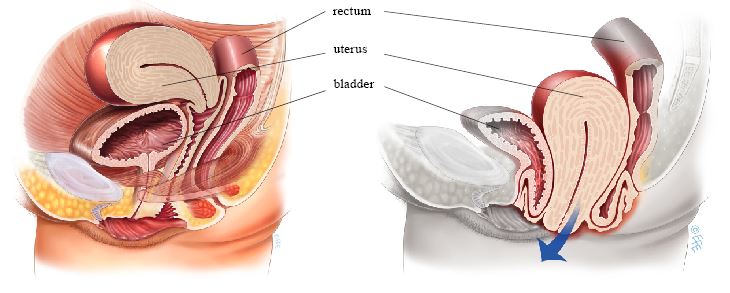
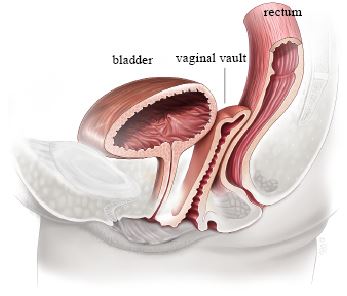
The uterus is detached from its supporting structures and removed through the vagina. A suspension procedure may be performed to support the vaginal apex. Removal of the uterus ends the ability to carry a pregnancy. The ovaries and fallopian tubes are separate structures: ovarian conservation and opportunistic removal of the fallopian tubes are discussed individually.
Recovery
- Hospital stay: typically 1-2 nights
- Return to light activities: 1-2 weeks
- Full recovery: approximately 6 weeks
- Sexual intercourse: usually after 8 weeks
- Light vaginal bleeding or spotting may occur for several days
Post-Operative Expectations
Following hysterectomy, menstrual periods will stop. If both ovaries are removed before natural menopause, surgical menopause occurs immediately; decisions about ovarian conservation should consider age, symptoms, cancer risk, and patient preference. All removed tissue is sent for pathology.
Risks and Expectations
For uterine prolapse, symptom and anatomical outcomes depend on the accompanying suspension and repairs, baseline prolapse, and length of follow-up. Prolapse can recur at the apex or in another compartment. Potential risks include:
- Previously hidden stress urinary incontinence — correcting a large prolapse can reveal leakage that was masked by urethral kinking
- Temporary urinary retention — may require a catheter while bladder emptying recovers
- Urinary tract infection
- Vaginal vault hematoma
- Bleeding — occasionally requiring transfusion
- Injury to bladder, ureters, or rectum — uncommon but may require repair
- Vaginal or pelvic infection — uncommon
- Venous thromboembolism — rare
Sources
Clinical content updated July 2026. Sources: ACOG: Hysterectomy and ACOG Committee Opinion: Opportunistic Salpingectomy.