Overview
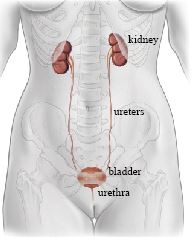
Urethral bulking involves injecting a biocompatible material around the urethra to improve its ability to close and reduce urine leakage during activities such as coughing, sneezing, or exercise.
When It May Be Considered
- Stress urinary incontinence confirmed by assessment
- Patients who prefer a less invasive option or wish to avoid mesh or abdominal tissue-harvest surgery
- Patients for whom a more invasive operation or anesthesia is less suitable
- Recurrent stress incontinence in selected cases
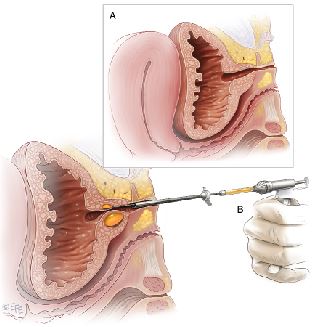
The Procedure
- Performed as an outpatient procedure under local anesthesia
- A cystoscope is used to guide injection of the bulking agent around the urethra
- The procedure takes approximately 15-30 minutes
- You can usually go home the same day
Effectiveness
- Improvement is generally less predictable and less durable than with sling or colposuspension surgery
- Symptoms may not resolve completely
- Benefit may diminish and repeat injections may be needed; timing varies
Advantages
- Minimally invasive with no incisions
- Short procedure time
- Can be performed under local anesthesia
- Low risk of complications
Limitations
- Less durable than sling surgery
- Often requires repeat treatments
- It may not provide enough improvement for patients seeking the most durable option
Risks and Expectations
Published outcomes vary by bulking product, patient population, definition of success, and follow-up. Potential risks include:
- Pain on urination — burning or stinging that typically resolves within 24-48 hours
- Temporary voiding difficulty — may require short-term catheterization
- Blood in the urine — may occur briefly after the procedure
- Urinary tract infection
- Migration of bulking material from the injection site — rare
- Granuloma formation — a localized tissue reaction at the injection site — rare
- Allergic reaction — rare
Sources
Clinical content updated July 2026. Source: AUA/SUFU Stress Urinary Incontinence Guideline.