Overview
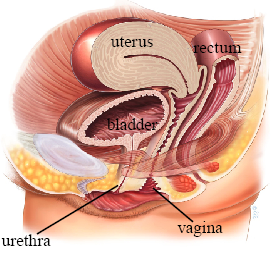
A midurethral sling is a permanent polypropylene mesh tape placed under the middle section of the urethra to provide support during activities that increase abdominal pressure (coughing, sneezing, exercise). It is an established surgical option for stress urinary incontinence, but it is not the only option.
Approaches
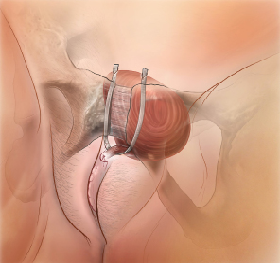
Retropubic Sling
The tape passes under the urethra through the retropubic space, exiting through two small skin incisions just above the pubic bone. This is the most studied approach with extensive long-term data.
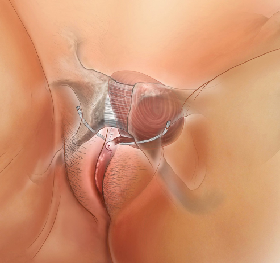
Transobturator Sling
The tape runs under the urethra and passes through the obturator foramen, exiting through small incisions in the groin creases. Effective with a slightly different risk profile (less risk of bladder injury, slightly higher risk of groin discomfort).
Both approaches can improve stress incontinence, but their risk profiles differ. Retropubic placement has a higher risk of bladder perforation and voiding difficulty; transobturator placement has a higher risk of groin or thigh pain. The choice should reflect anatomy, prior surgery, patient priorities, and surgeon experience.
The Procedure
- Performed under general or regional anesthesia
- Small incision in the vaginal wall beneath the urethra
- Sling positioned tension-free beneath the mid-urethra
- Typically a day-surgery procedure
- Procedure time: approximately 20-30 minutes
Recovery
- Most women recover within 2-4 weeks
- Some groin discomfort (especially with transobturator) may last a couple of weeks
- Light vaginal bleeding for 7-10 days is not unusual
- Return to full activity including exercise: approximately 4-6 weeks
Important Information
This procedure is designed to treat stress incontinence. It is not a treatment for urgency incontinence or overactive bladder. Pre-existing urgency may improve, remain unchanged, or worsen, and new urgency can develop.
The mesh implant is intended to remain permanently. Mesh exposure, infection, pain, voiding difficulty, or injury may require further treatment. Partial or complete mesh excision can be difficult, may not remove every symptom, and complete removal may not be possible without injury.
Non-mesh alternatives include pelvic floor physiotherapy, urethral bulking, Burch colposuspension, and an autologous fascial sling. These options have different effectiveness, recovery, and risks.
Risks and Expectations
Many patients have substantial improvement, but published results vary by sling route, patient population, definition of success, and follow-up duration. Potential risks include:
- Mesh exposure — may present weeks, months, or years after surgery and may require treatment
- Voiding difficulty — usually temporary but may require catheterization, sling release, or another procedure
- Bladder or urethral injury — bladder perforation is more associated with the retropubic route; cystoscopy is used to check placement
- New or worsened urgency
- Pain — including pelvic pain and route-specific groin or thigh pain
- Urinary tract infection — common in the early post-operative period
Sources
Clinical content updated July 2026. Source: AUA/SUFU Stress Urinary Incontinence Guideline.