Overview
Sacrocolpopexy is a surgical procedure that suspends the vaginal apex (or the uterus/cervix in uterine-preserving approaches) to the sacrum (a bone at the base of the spine) using synthetic mesh. A laparoscopic approach may offer a shorter recovery than open abdominal surgery, although individual recovery varies.
Why Sacrocolpopexy?
Sacrocolpopexy can provide durable apical support and is one established option alongside native-tissue vaginal or laparoscopic repairs, uterus-preserving procedures, pessary management, and colpocleisis. It may offer greater anatomical durability in some comparisons, but it requires an abdominal operation and introduces permanent mesh-specific risks.
Indications
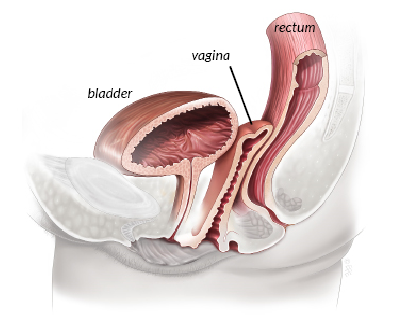
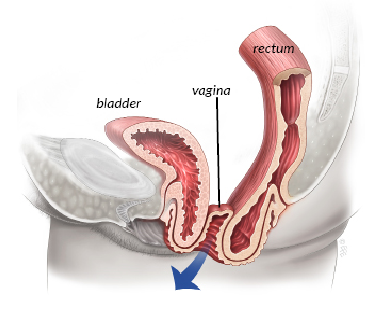
- Symptomatic apical (vault or uterine) prolapse
- Recurrent prolapse after prior vaginal repair
- Women who wish to maintain sexual function
- Patients suitable for general anesthesia and a laparoscopic approach
The Procedure
- Performed through small abdominal incisions under general anesthesia
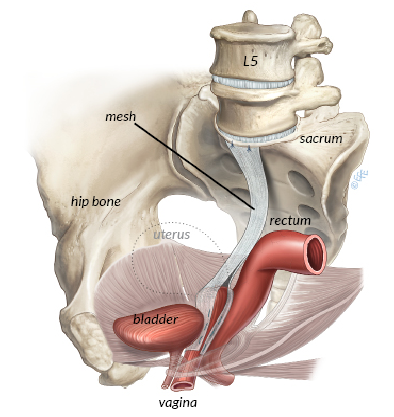
- A lightweight polypropylene mesh is attached to the front and/or back wall of the vagina
- The mesh is then secured to the sacral promontory (a bony landmark on the sacrum)
- The peritoneum is closed over the mesh to reduce contact with the bowel
May be combined with other procedures such as anterior or posterior repair, anti-incontinence surgery, or hysterectomy if indicated.
Recovery
- Hospital stay: typically 1-2 nights
- Return to light activities: 2-3 weeks
- Full recovery: approximately 6 weeks
- Sexual intercourse: usually after 8 weeks
Considerations
- The polypropylene mesh is intended to remain permanently. Exposure, infection, pain, or erosion into an organ may require further surgery; complete removal may be difficult or impossible without injury.
- Longer surgery compared to vaginal approaches
- Small risk of injury to surrounding structures
- Not suitable for all patients — the choice between sacrocolpopexy and vaginal repair is individualized
Risks and Expectations
Outcomes vary depending on whether success means relief of bulge symptoms, anatomical support, avoidance of retreatment, or sexual and urinary function, and on the length of follow-up. Surgery does not guarantee a permanent cure. Potential risks include:
- Mesh exposure, infection, contraction, or erosion — may occur early or years later and may require another procedure
- Voiding difficulty — usually temporary but may require short-term catheterization
- Pain or discomfort during intercourse
- Constipation or bowel dysfunction
- Injury to bladder, bowel, ureters, blood vessels, or nerves
- General surgical risks — including urinary tract infection, wound infection, bleeding requiring transfusion, and venous thromboembolism
Sources
Clinical content updated July 2026. Sources: NICE Guideline: Urinary Incontinence and Pelvic Organ Prolapse in Women and AUGS Patient Resources.