Overview
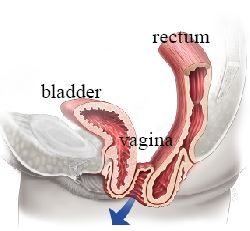
Apical suspension procedures support the top of the vagina (vaginal vault) or the uterus/cervix by anchoring them to strong ligaments or bony structures within the pelvis. These are essential components of prolapse surgery, as adequate apical support is the foundation of a durable repair.

Uterosacral Ligament Suspension
The vaginal apex or cervix is sutured to the uterosacral ligaments — strong native ligaments that naturally support the uterus. This can be performed vaginally or laparoscopically.
Advantages:
- Uses native tissue (no mesh)
- Re-establishes the natural axis of the vagina
- Can be combined with other vaginal repairs
Considerations:
- Risk of ureteral kinking or injury; cystoscopy is used to check ureteral function
- Cystoscopy is routinely performed during the procedure to confirm ureteral function
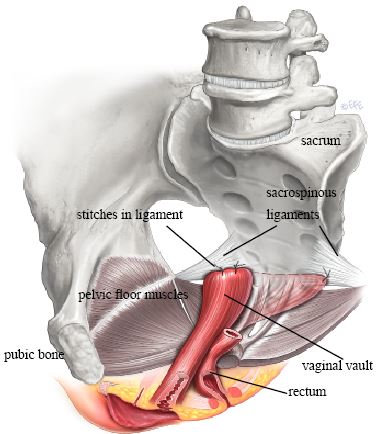
Sacrospinous Ligament Fixation
The vaginal apex is sutured to the sacrospinous ligament, a strong ligament deep in the pelvis. This is performed through a vaginal approach.
Advantages:
- No abdominal incisions
- Well-established procedure with good long-term results
- Particularly useful in combination with vaginal hysterectomy
Considerations:
- May result in a slightly posterior deviation of the vaginal axis
- Temporary buttock or leg pain may occur due to proximity to nerves (usually resolves within weeks)
Laparoscopic Sacrocolpopexy / Colposacropexy
Sacrocolpopexy, sometimes called colposacropexy, is an abdominal or laparoscopic apical suspension procedure where a strip of surgical mesh is attached to the top of the vagina and secured to the sacrum. It is often considered for recurrent or advanced apical prolapse, especially when long-term anatomic durability is a priority and the patient is suitable for a laparoscopic approach.
This procedure avoids a vaginal mesh incision but does use permanent mesh inside the abdomen, so counselling includes mesh-specific risks such as exposure or erosion, as well as the usual surgical risks. More detail is available on the laparoscopic sacrocolpopexy page.
Recovery
- Hospital stay: typically 1-2 nights
- Return to light activities: 1-2 weeks
- Full recovery: approximately 6 weeks
Risks and Expectations
Outcomes depend on the operation, baseline prolapse, associated repairs, definition of success, and length of follow-up. No approach guarantees permanent correction. The specific risk profile depends on the technique used.
Sacrospinous fixation:
- Buttock or leg pain — usually improves, but persistent nerve-related pain is possible
- New stress urinary incontinence — correction can reveal leakage that was previously masked by prolapse
- Voiding difficulty — may require temporary catheterization or further treatment
Uterosacral ligament suspension:
- Ureteric kinking or injury — intraoperative cystoscopy is used to check urine flow from both ureters
- Urinary tract infection — risk is higher when a catheter is used
- Buttock pain — usually short-term
Common risks for both procedures:
- Prolapse recurrence or development in another compartment
- Dyspareunia — rare; most women report improved sexual function
- Bleeding requiring transfusion — uncommon
- Venous thromboembolism — rare
Sources
Clinical content updated July 2026. Source: NICE Guideline: Urinary Incontinence and Pelvic Organ Prolapse in Women.