Overview
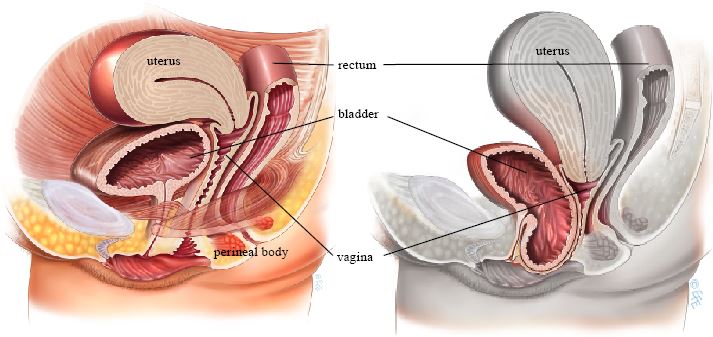
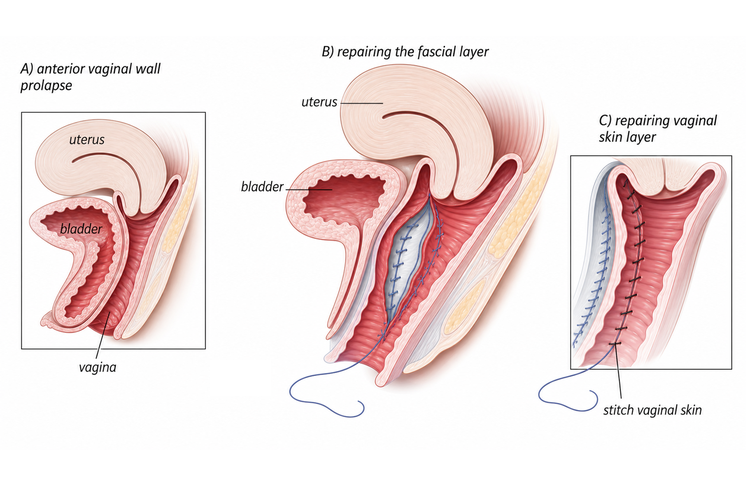
Anterior colporrhaphy (anterior repair) is a vaginal surgical procedure used to correct prolapse of the front wall of the vagina (cystocele), where the bladder bulges into the vaginal canal. The procedure uses the patient's own tissue (native tissue repair) to restore support.
Indications
- Symptomatic anterior compartment prolapse (cystocele)
- Vaginal bulge causing discomfort, pressure, or urinary symptoms
- Difficulty emptying the bladder due to prolapse
The Procedure
An incision is made in the front wall of the vagina. The tissue between the vagina and the bladder (pubocervical fascia) is identified and plicated (folded and reinforced with stitches) to strengthen the support beneath the bladder. Excess vaginal tissue may be trimmed, and the incision is closed with absorbable sutures.
Advantages
- No synthetic mesh — uses your own tissue
- Performed vaginally with no abdominal incisions
- Shorter operative time compared to abdominal approaches
- Faster initial recovery
Recovery
- Hospital stay: typically 1 night
- Return to light activities: 1-2 weeks
- Full recovery: approximately 6 weeks
- Sexual intercourse: usually after 8 weeks
- Avoid heavy lifting for 6 weeks
Risks and Expectations
Outcomes vary depending on whether success means relief of bulge symptoms, anatomical support, improved emptying, or avoidance of repeat treatment, and on the length of follow-up. As with any surgical procedure, there are potential risks:
- Prolapse recurrence — prolapse may return or develop in another vaginal compartment over time, potentially requiring further surgery
- Urinary tract infection — more common when a catheter is used
- New stress urinary incontinence — may develop after large repairs if correction of the prolapse unkinks the urethra
- Dyspareunia — some women may experience discomfort during intercourse after surgery
- Constipation — a common short-term post-operative issue
- Bleeding — occasionally requiring transfusion
- Bladder or ureteral injury — uncommon but possible during surgery
Anterior repair is often combined with apical suspension and/or posterior repair. The choice between approaches is individualized based on patient factors and surgeon recommendation.
Sources
Clinical content updated July 2026. Source: NICE Guideline: Urinary Incontinence and Pelvic Organ Prolapse in Women.