What is Pelvic Organ Prolapse?
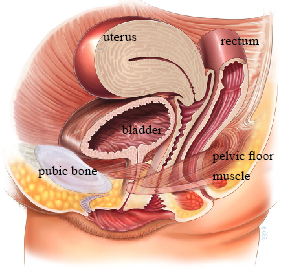
Pelvic organ prolapse (POP) occurs when the pelvic floor muscles and fascia (a network of supporting tissue) that hold the pelvic organs in their correct positions become weakened. This allows one or more pelvic organs — the bladder, uterus, or rectum — to descend into or beyond the vaginal canal.
POP is a very common condition. Up to 50% of women who have had children will have some degree of prolapse, though many have minimal or no symptoms. It is important to emphasize that only about 1 in 9 women (11%) will ever need surgery for prolapse in their lifetime.
Symptoms
Symptoms of pelvic organ prolapse include:
- A heavy dragging feeling in the vagina or lower back
- Feeling of a lump in or outside the vagina
- Urinary symptoms such as a slow urinary stream, incomplete bladder emptying, urinary frequency or urgency, and stress incontinence
- Bowel symptoms such as difficulty with bowel movements, incomplete emptying, or needing to press on the vaginal wall to evacuate
- Discomfort during sexual intercourse
Causes and Risk Factors
The main cause of prolapse is damage to the nerves, ligaments, and muscles which support the pelvic organs:
- Pregnancy and childbirth are major contributing factors and may cause weakening of the vagina and its supports. A prolapse may occur during or shortly after pregnancy or may take many years to develop.
- Aging and menopause may cause further weakening of pelvic floor structures due to declining estrogen levels.
- Conditions causing excessive pelvic pressure such as obesity, chronic cough, chronic constipation, and repetitive heavy lifting.
- Genetic predisposition: Some women may have an inherited risk for prolapse, while connective tissue disorders such as Marfan syndrome and Ehlers-Danlos syndrome can also contribute.
Types of Prolapse
Prolapse is classified by which compartment is involved. Many women have prolapse in more than one compartment.
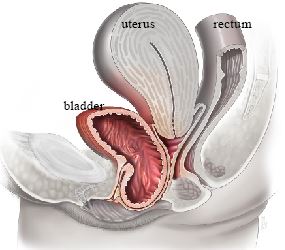
Anterior Compartment Prolapse (Cystocele)
The bladder and/or urethra bulge into the front wall of the vagina. This is the most common type of prolapse.
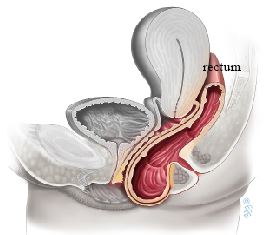
Posterior Compartment Prolapse (Rectocele)
The rectum bulges into the back wall of the vagina, or part of the small intestine may bulge into the upper back wall (enterocele).
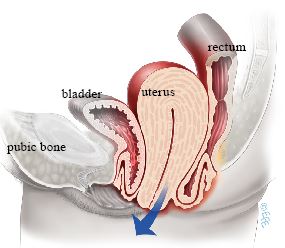
Apical Prolapse
- Uterine prolapse: The uterus drops or herniates into the vagina. This is the second most common form.
- Vaginal vault prolapse: Following hysterectomy, the top of the vagina may collapse downward, falling toward or out of the vaginal opening.
Grading Prolapse Severity
Your physician will perform a vaginal examination to determine prolapse severity. The Pelvic Organ Prolapse Quantification (POP-Q) system grades prolapse from Stage 1 (mild) to Stage 4 (complete eversion). The degree of prolapse seen on examination does not always correlate with symptom severity.
Non-Surgical Treatment Options
Conservative management may be appropriate for women with mild or moderate symptoms, or those who prefer to avoid surgery.
- Observation: Appropriate if symptoms are minimal or absent. Try to avoid heavy lifting, chronic straining, and excess weight gain, as these can worsen prolapse.
- Pelvic floor physiotherapy: Supervised exercises to strengthen the pelvic floor muscles can improve or prevent worsening of early-stage prolapse. Maximum benefit usually occurs after 3 to 6 months of regular exercise.
- Pessary: A removable silicone device inserted into the vagina to provide mechanical support for prolapsed organs. Pessaries can be used temporarily or long-term and it is possible to remain sexually active with some types.
- Lifestyle modification: Weight management, avoidance of heavy lifting, and treatment of chronic cough or constipation.
Surgical Treatment Options
For women with symptomatic prolapse, surgical repair may be offered. The approach depends on age, previous surgical history, severity, and individual preferences.
Native Tissue Vaginal Repairs
These procedures use the patient's own tissue to restore support and are performed through the vagina:
- Anterior colporrhaphy (bladder support)
- Posterior colporrhaphy (rectal support)
- Uterosacral ligament suspension
- Sacrospinous ligament fixation
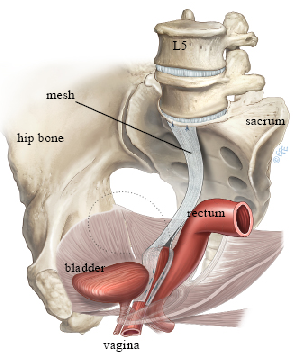
Sacrocolpopexy (Laparoscopic)
A minimally invasive abdominal procedure that suspends the vaginal apex to the sacrum using permanent synthetic mesh. It may provide greater anatomical durability in some settings, but mesh-specific risks and the longer abdominal procedure must be weighed against native-tissue options.
Colpocleisis (Vaginal Closure)
Closes most or all of the vaginal canal to support prolapsed organs. It is an option for patients who do not want future vaginal penetration and may offer a shorter operation than reconstructive procedures. It prevents vaginal penetration but does not eliminate external sexual sensation, intimacy, or orgasm. The decision is permanent and requires careful counselling.
Choosing an Operation
There is no single best prolapse operation for everyone. Outcomes vary depending on whether success means relief of bulge symptoms, anatomical support, avoidance of repeat treatment, or sexual and urinary function, and also on length of follow-up. Native-tissue repair, uterus-preserving repair, mesh sacrocolpopexy, and colpocleisis are all legitimate options for appropriately selected patients. Future pregnancy can place a repair under strain, so timing should be discussed when childbearing is not complete.
When to Seek Help
If you are experiencing symptoms of pelvic organ prolapse, Dr. Kruger can provide a comprehensive evaluation and discuss which treatment options are most appropriate for your specific needs.
Sources
Clinical content updated July 2026. Sources: AUGS Patient Resources and NICE Guideline: Urinary Incontinence and Pelvic Organ Prolapse in Women.