What is Fecal Incontinence?
Fecal incontinence is the loss of control over bowel movements, resulting in the leakage of gas or stool through the anus. The severity can range from difficulty controlling gas to loss of control over liquid or formed stool. It is common and often under-reported.
Fecal incontinence can be distressing and severely affect everyday life. Many people find it difficult and embarrassing to discuss with healthcare professionals, yet once identified, treatment can often reduce symptoms and improve daily function.
How Does Normal Bowel Control Work?
Normal bowel frequency varies from three times a day to twice a week, but most people have a bowel movement once daily. The bowel and rings of muscle around the back passage (anal sphincter) work together to ensure bowel contents are not passed until you are ready.
The sphincter has two main muscles:
- Internal anal sphincter — keeps the anus closed at rest
- External anal sphincter — provides extra protection when the urge to open the bowel is felt and when we cough or sneeze
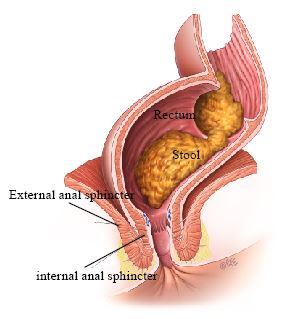
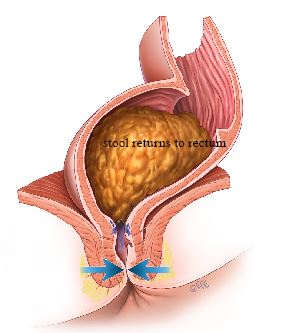
When stool enters the rectum, the internal sphincter automatically relaxes to allow sensitive nerves at the top of the anal canal to detect whether it is gas, liquid, or solid stool. The external sphincter can be deliberately squeezed to delay bowel emptying, pushing stool back into the rectum until a convenient time.
Causes
One of the most common causes in women is injury during childbirth. The anal muscles may be torn during delivery, or there may be damage to the nerves that help the anal muscles function. Some injuries are recognized at the time of delivery, but others may not be obvious and only become a problem later in life.
Other causes include:
- Age-related loss of muscle strength
- Anal surgery or injury
- Inflammatory Bowel Disease or Irritable Bowel Syndrome
- Nerve damage from childbirth, diabetes, or neurological conditions
- Pelvic radiation therapy
- Rectal or pelvic organ prolapse
Evaluation
Assessment includes discussion of your symptoms, their severity, and their impact on your lifestyle. Important factors include:
- Childbirth history (multiple births, large babies, instrumental deliveries, episiotomy or tears)
- Physical examination including assessment of the anal sphincter
- Endoanal ultrasound — provides a picture of the sphincter muscles and can identify disruption or defects
- Anal manometry — measures the pressure and strength of the sphincter muscles
- Additional tests as needed, depending on the clinical situation
Treatment Options
Self-Help Measures
- Diet and bowel habits: Eat a healthy balanced diet, drink 1.5-2 liters of fluid per day. Keep caffeinated drinks to a minimum. Experiment with your diet to identify foods that worsen symptoms. Establish regular bowel habits, ideally using the toilet after meals.
- Correct toilet positioning: Use a footstool to elevate your feet, which helps with bowel emptying. Avoid straining.

- Skin care: Wash gently with warm water after bowel movements, pat dry gently, and use non-scented products to prevent skin irritation.
Pelvic Floor and Sphincter Exercises
Specialized exercises to strengthen the pelvic floor and anal sphincter muscles can improve bowel control. Biofeedback techniques can retrain the bowel to be more sensitive to the presence of stool, and electrical stimulation may be used to improve muscle coordination and strength.
Medications
Medications may help when the bowel is overactive, when stool is very loose, or when the sphincter muscles are weak. Drugs can decrease bowel activity, making stool more formed and the sphincter tighter.
Nerve Stimulation
Tibial nerve stimulation uses a small needle near the ankle to stimulate nerves involved in bowel function. Evidence for fecal incontinence is mixed, so expected benefit and alternatives should be discussed before treatment.
Sacral Neuromodulation
For persistent symptoms, a device can be implanted to directly stimulate the nerves controlling bowel function. This is reserved for cases that have not responded to other treatments.
Surgical Options
Sphincter repair or reconstruction may be considered when there is a defined structural defect in the anal sphincter muscles.
Sources
Clinical content updated July 2026. Source: American Society of Colon and Rectal Surgeons Clinical Practice Guideline for the Management of Fecal Incontinence (2023).